Bronchiectasis
Overview
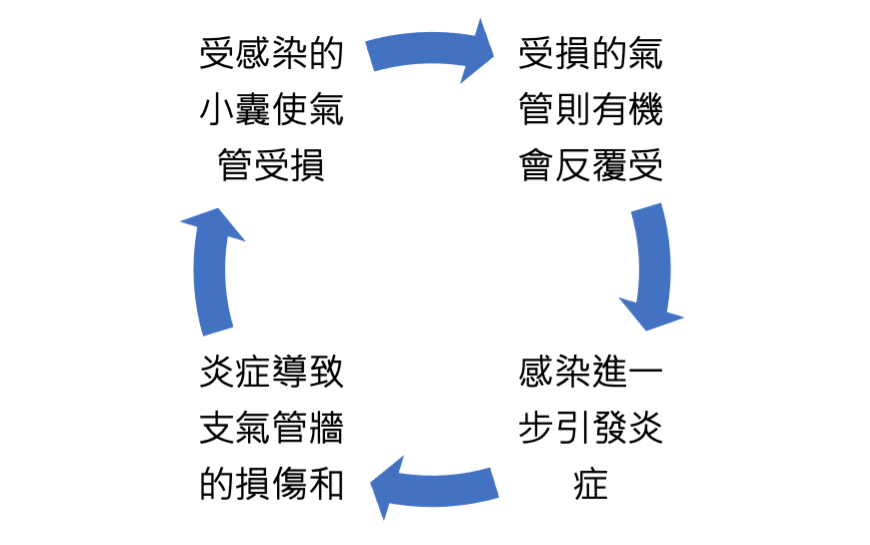
Bronchiectasis is a chronic condition in which the bronchi become permanently widened and the bronchial walls are damaged. In a healthy state, the airways guide the air we breathe into the lungs. However, in bronchiectasis, some bronchi become deformed and enlarged, forming small sacs where bacteria and mucus accumulate, leading to infection. The cilia inside the bronchi are also damaged, making them unable to effectively clear mucus from the lungs.
This creates a vicious cycle: repeated infections cause inflammation and airway damage, which in turn leads to more infections, ultimately resulting in persistent bronchial dilation and destruction.

Causes / Risk Factors
- Previous severe lung infections
- Inherited diseases such as cystic fibrosis
- Conditions affecting airway cilia (e.g. primary ciliary dyskinesia)
- Previous pulmonary tuberculosis
- In many patients, no clear cause is identified
Common Symptoms
- Chronic cough with large amounts of thick sputum, sometimes streaked with blood
- Increased coughing and sputum production in the morning or when lying down at night
- Persistent chest tightness, breathlessness, or wheezing
- Marked increase in yellow-green sputum during acute respiratory infections
- Recurrent lung infections and haemoptysis; in severe cases, significant weight loss and breathlessness
- Clubbing: swelling and deformity of the fingertips
Diagnosis
- Medical history and physical examination: Doctors will ask about symptoms and medical history, followed by a physical examination to look for signs suggestive of bronchiectasis.
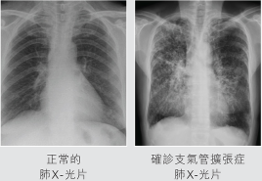
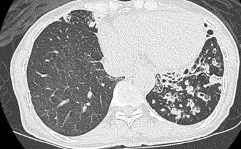
- Imaging: A chest X-ray may show abnormalities, but a CT scan of the lungs is the most accurate method for diagnosis.
- Lung function tests: These help determine the severity of bronchiectasis and rule out other conditions with similar symptoms.
- Sputum tests: Used to identify bacteria or other micro-organisms causing infection, guiding treatment.
- Blood tests: Assess immune function and help exclude other possible causes.
Treatment and Management
Prevention of Infections
- Patients with bronchiectasis should make lifestyle adjustments to support long-term health management.
Vaccinations
- Vaccines such as influenza and pneumococcal vaccines help prevent infections that can worsen bronchiectasis. Good personal hygiene is essential: wash hands frequently, and rinse or brush teeth after meals and before bed to reduce oral bacteria that may trigger respiratory infections.
Pulmonary rehabilitation
- A programme combining exercise, education, and support to help patients manage their condition.
Diet
- Maintain a balanced diet with nutrient-rich foods. Avoid spicy, overly salty, or greasy foods. High-calorie, high-protein, and vitamin-rich foods can help strengthen the body and improve immunity.
Avoid smoking and alcohol
- Quit smoking and avoid second-hand smoke. Reduce alcohol intake to minimise airway irritation.
Can bronchiectasis be cured?
Once the bronchi are permanently widened and damaged, they generally cannot return to normal.
Treatment aims to control symptoms, reduce exacerbations, preserve lung function, and maintain quality of life.
1. Airway Clearance Techniques
These techniques have gained significant clinical importance and are proven to improve symptoms. Methods include:
- Respiratory physiotherapy: ideally guided by a trained respiratory therapist
- Active Cycle of Breathing Technique (ACBT)
- Autogenic drainage
- Positive pressure devices, such as PEP masks and oscillating PEP devices (e.g., Flutter, Acapella)
Postural drainage combined with chest vibration or percussion is also commonly used.
Regular exercise (walking, cycling, swimming) helps clear secretions and improve lung function.
Airway clearance is often more effective than simply increasing medication, but requires daily commitment for best results.
2. Long-term Low-dose Macrolide Antibiotics
Recent studies show macrolides can:
- Reduce the number of acute exacerbations
- Provide anti-inflammatory and immune-modulating effects beyond antibacterial action
Suitable for patients who:
- Have 2–3 or more exacerbations per year
- Continue to have flare-ups despite good airway clearance
- Have been assessed for non-tuberculous mycobacterial (NTM) infection
Before starting treatment, doctors may assess:
- ECG (QT interval)
- Liver function
- Sputum culture for NTM
- Hearing status
3. Inhaled Antibiotics
Increasingly important for patients with recurrent infections, especially those with Pseudomonas aeruginosa.
Advantages:
- Direct delivery to the lungs with high local concentration
- Fewer systemic side effects
Suitable for:
- Multiple exacerbations within a year
- Persistent Pseudomonas or other difficult-to-treat bacteria in sputum cultures
4. Bronchodilators and Inhaled Steroids
Used only when patients also have:
- Asthma
- Asthma-like features
- COPD (Chronic Obstructive Lung Disease)
- Airway hyperreactivity or reversible airflow obstruction
Common medications include:
- Long-acting bronchodilators (LABA, LAMA, LABA+LAMA)
- LABA + inhaled corticosteroid (ICS) combinations
5. Treating Comorbidities and Reversible Causes
- Sinusitis / nasal polyps: treating these can reduce lower airway infections
- Gastro-oesophageal reflux or aspiration: consider if night-time cough or recurrent pneumonia occurs
- Immune deficiency: some patients may require immunoglobulin replacement
6. Surgical or Interventional Treatment
(Only for selected severe cases)
- Lung resection or bronchial artery embolisation (BAE) may be considered for localised disease with recurrent severe haemoptysis or infection
- Lung transplantation may be evaluated for end-stage disease with severe lung failure
Latest Advances in Bronchiectasis Treatment
In August 2025, the US FDA approved Brensocatib, the world’s first targeted therapy specifically for non-cystic fibrosis bronchiectasis.
- Mechanism: a DPP-1 inhibitor that blocks activation of neutrophil proteases, reducing chronic airway inflammation and tissue damage
- Clinical benefits: once-daily oral treatment significantly reduced acute exacerbations by 21%, slowed lung function decline, and improved quality of life
Please consult your doctor for all treatment decisions.
Last updated: March 2026